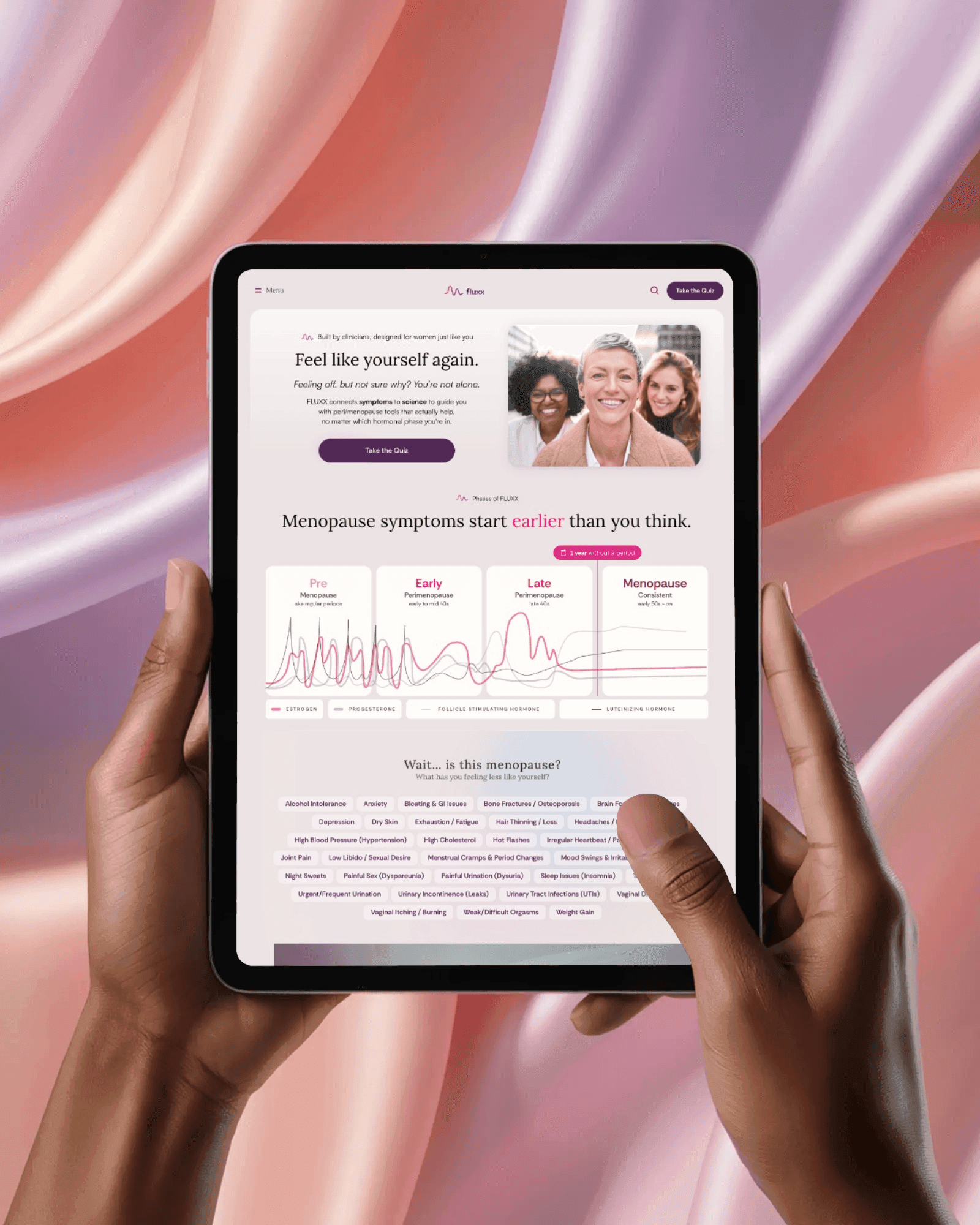
Launching FLUXX: An AI-Powered Menopause Platform
Healthcare0-to-1 MVPAI / MLProduct Strategy
"Kate took an overwhelming, high-emotion space and made it navigable. We had clarity on what to build, why it mattered, and how to launch without losing user trust." - FLUXX Founder
The impact
MVP live in under 6 months. 47% engagement. 800+ quiz completions. 38% reduction in quiz abandonment. Organic search nearly tripled month over month.
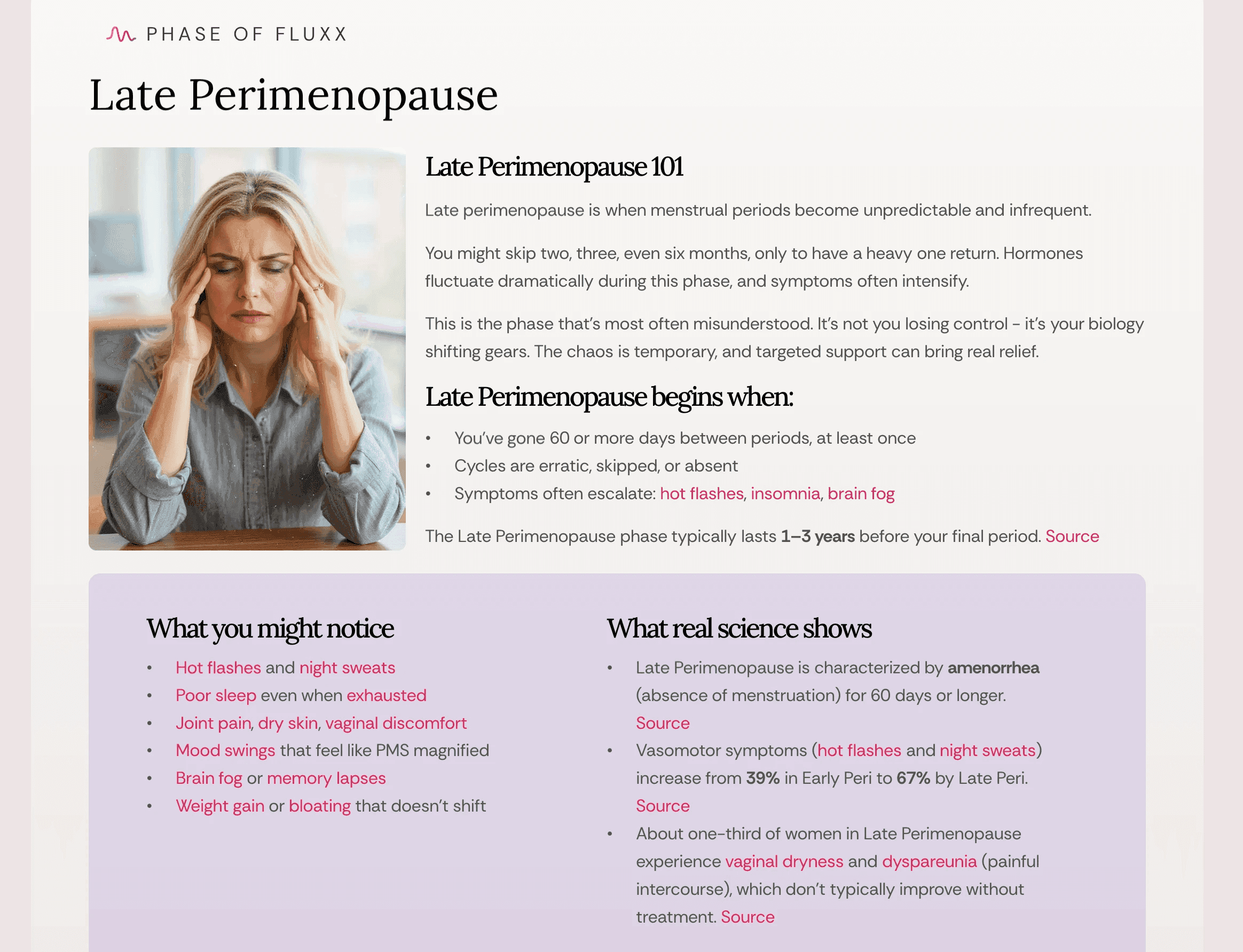
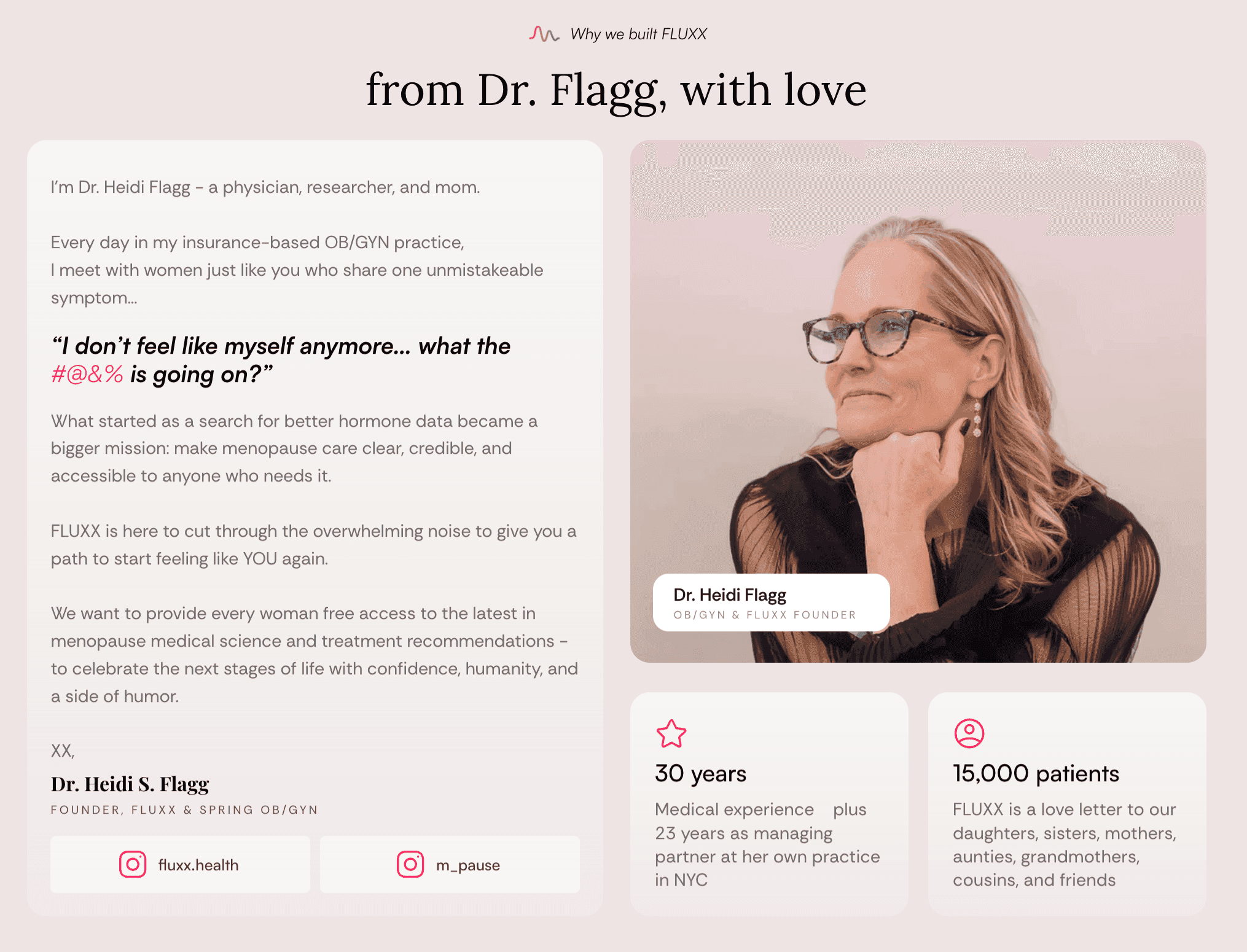
Those engagement numbers sit above what is typical for early healthtech, where most education apps struggle to get past a single session. The reason is not the AI. It is that the product earned enough trust for people to come back to a topic most of them had been dismissed about for years. FLUXX went from clinical research with no delivery system to a working product with 120 active users, 30+ symptom education pages, and a phase-based AI scoring engine validated by real clinicians (founder Dr. Flagg and Dr. Aoife O'Sullivan), with an AI-simulated clinician panel doing the cheap first-pass review.
The hard part wasn't the AI
When I joined, FLUXX had a founder with deep clinical expertise and a strong mission, but no product infrastructure. Ideas lived in conversations. There was no backlog, no delivery cadence, and no shared definition of "MVP."
The real constraint was sharper than "no process." Menopause education sits one wrong sentence away from medical advice. The product had to be clinically credible and emotionally safe and stay legally on the education side of a line that a diagnosis would cross. A generalist plan that optimized for shipping features fast would have shipped the company straight into that line. The work was to build a system that moved quickly because it had guardrails, not despite them.
So I started by narrowing, not building. I defined three parallel bets, a phase-aware quiz engine, clinician enablement, and monetization experiments, and put them on a now / next / later roadmap. That single framing stopped the team from chasing every good idea at once and made it obvious what we were deliberately not doing yet. We moved task management into Linear and replaced ad hoc, founder-driven decisions with weekly async rituals the team could run without me in the room.

Making clinical trust cheap to earn
The highest-leverage decision was how to handle clinical trust. The obvious move in healthtech is a logo wall of advisors. I built the opposite: an AI-simulated clinician panel that pre-screened every recommendation before any real clinician spent a minute on it. Real clinical input came from founder Dr. Heidi Flagg (OB-GYN) and Dr. Aoife O'Sullivan plus a few of Dr. Flagg's colleagues; to pressure-test content at the speed an MVP needs, I designed GPT + NotebookLM personas of leading public menopause voices as an internal validation layer.
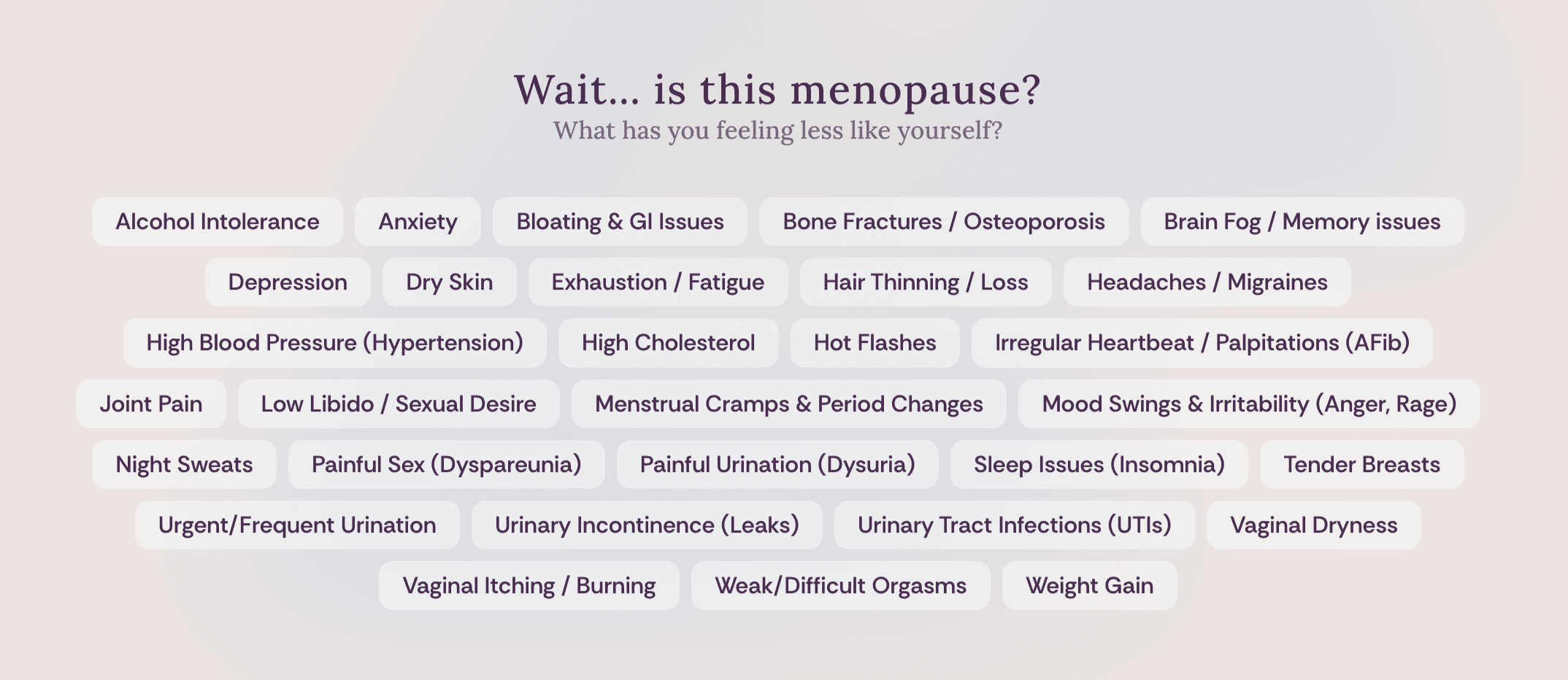
That let me solve the scoring problem honestly. Designing recommendation logic across 150+ symptom types and multiple hormonal phases is not hard to build; it is hard to make safe. I built prompt-based scoring with the founder, then created a 5-step clinical validation process using GPT and NotebookLM to simulate a clinician panel review on quiz outputs before any human clinician spent time on them. The simulation caught the obvious failures cheaply so the real clinicians could focus on the subtle ones. Every recommendation routed to a "What to Ask Your Doctor" prompt, which kept the product firmly in education and out of diagnosis by design, not by disclaimer.

Trust is a retention mechanism, not a feature
Menopause is personal, variable, and routinely mishandled in digital health. So the UX had to do emotional work, not just functional work. I designed trauma-aware language systems and mobile-first flows that lowered the cost of a first, vulnerable interaction, and built re-engagement on intent-based CTAs rather than guilt-driven notifications.
That distinction is why the 47% engagement number matters. It did not come from nagging people back. It came from giving them a reason to return, which is the only kind of engagement that compounds in a sensitive health product. Routing recommendations through real clinicians instead of a logo wall of advisors was the same bet in another form: a genuine feedback loop instead of a credibility prop.

What this built
- A delivery system the team can run without me. Sprint rituals, a structured backlog, and cross-functional patterns that replaced founder-driven decisions with repeatable delivery.
- A clinically validated AI scoring engine. Phase-based recommendations with traceable logic that clinicians can audit and patients can trust, kept on the right side of the education line by design.
- A monetization roadmap grounded in real data. 50+ ideas across 7 revenue categories, sequenced by phase-based kits and real willingness to pay rather than guesswork.
Sources
- Janna Bastow, "Now-Next-Later Roadmaps" via ProdPad -- roadmap framing adapted to sequence FLUXX's three parallel bets
Resources & artifacts
LinkFLUXX Health -- Live Product
Menopause education platform with phase-based quiz, 30+ symptom pages, and clinician-backed recommendations.
Case StudyUsing AI to Validate Clinical Recommendations
Case study summary: multi-phase clinical validation process combining expert review with structured QA, scoring AI-generated menopause education content across accuracy, completeness, and clinical nuance.
PDF
PRD: Digital Symptom Tracker
PRD summary: symptom tracker MVP covering daily logging, trends dashboard, and provider visit summaries for the menopause education platform.
The thinking behind this work
Experiment-Driven Development
The cheapest experiment that could change your mind is worth more than the most sophisticated feature nobody asked for.
Getting Unstuck
Every team gets stuck. The difference is whether you have a framework to diagnose why and a playbook to get moving again.
The Live Whiteboard Method
A repeatable six-move method for live whiteboarding, drawn from real PM interviews and client working sessions. The board is not a finished artifact. It is a legible argument that builds in real time.
Services behind this work
Related case studies
Designing a Wellness MVP for Biomarker-Driven Preventative Care
Director of Product (Fractional) · 2024 - 2025
Served as Fractional Director of Product to lead Sperity Health from vaporware to a functioning, HIPAA-compliant MVP. Built the roadmap, treatment logic, product team, and app experience for members to understand diagnostics, track progress, and access elite care.
Stanza MVP: FDA-Cleared CBT App for Fibromyalgia
Senior Product Manager · 2019 - 2020
Launched regulated CBT app MVP with evidence-backed design, tracking, and patient onboarding.
A Tinkerer's Workbench
PM, Designer, & Engineer · 2024-2026
26+ free apps built end-to-end: PM assessments, AI diagnostics, a daily puzzle game, recipe tools, travel utilities, and more. Real products, not demos.
Want to bring this kind of thinking to your team?
I help teams ship products with clarity, speed, and care.
Or trace the through-line: the full 14-year career timeline →